The Current Health Care "Reform" Legislation:
How it will make rationing
and death hastening
the law of the land
11/23/09
Ione Whitlock
In Progressive politics, Death frequently comes in
packages labeled “Life.”
And so it is with legislation such as that which is now
before the Senate. Think you are
supporting pain relief and hospice legislation in order to prevent assisted
suicides? Wrong. Thanks to Big Death — a collection of
heavily funded non-profit hospice and palliative care groups[i] — the line between palliative care (pain
relief; symptom management) and imposed death has become blurred.
One Big Death “thought leader” who has helped create the
confusion between life-affirming palliative care and imposed death is Ira Byock,
Dartmouth
physician and hospice guru. In a blog at the New America Foundation[ii] this summer, he illustrated our point. He suggests, using the example of one
senior citizen, that we might improve seniors’ lives simply by giving them
“reliable transportation … to the local
Senior
Center [where they would] share nutritious
group lunches and noon-time discussions on advance directives for health
care”. In other words, he wants to
sell seniors a free trip to the Center for a fulfilling and healthy life … to
persuade them to focus on death, of course.
Byock drew early attention and support from Andrea Kydd –
former organizer for the Welfare Rights Organization, and board member of the
Tides Foundation. Kydd, who was
health program director for the Nathan Cummings Foundation, directed the
foundation's support to two end-of-life projects in 1995: one collaborated with the Commonwealth
Fund to conduct a caregiver study directed by Ezekiel Emanuel and his wife
Linda; the other was Byock’s Missoula Demonstration Project. The grant from Cummings was followed by
a grant from Soros – one of the earliest grants awarded in Soros’s Project on
Death in
America
.
From there Byock moved to projects sponsored by the
Robert Wood Johnson Foundation. He directed a massive $15 million end-of-life
project “Promoting Excellence” that could have been called “Promoting
Rationing.” 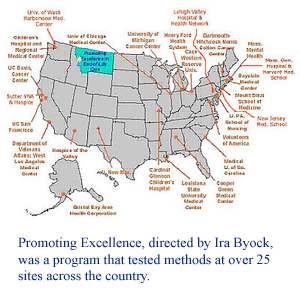 It tested methods of
“moving hospice upstream” in various “difficult” clinical settings and on
specific populations: veterans hospitals, native American reservations, African-Americans in
urban centers, and prisons, for example. The project, headquartered in
Montana, focused on financial savings and
various ways to convince people to accept “palliative care” earlier in the
game. It tested methods of
“moving hospice upstream” in various “difficult” clinical settings and on
specific populations: veterans hospitals, native American reservations, African-Americans in
urban centers, and prisons, for example. The project, headquartered in
Montana, focused on financial savings and
various ways to convince people to accept “palliative care” earlier in the
game.
Blurring the distinction between life-affirming care and
hastened death eases the path for bedside rationing, which of course lowers
costs. How to convince “difficult”
cases to forgo life-sustaining treatment? Offer them palliative care.
When Promoting Excellence moved to South
Carolina, the effort was focused on reminding a group of chronically ill
patients who “generally do not see themselves as dying” that, in fact, they were
dying. Diane Meier and Sean
Morrison of
Mt.
Sinai in
New
York worked with NJ-based Franklin Health and Blue Cross
Blue Shield of South Carolina for intervention by case management teams using
advance care counseling and a variety of other tools. Meier’s group reported that the
South Carolina population were “an ‘upstream’ population of very sick people,
averaging 46 years of age, generally suffering from serious, progressive, and
life threatening illnesses, who will likely consume high dollar amounts of
resources” and were thus chosen for intervention.
When Byock delivered a provocative keynote address to
a conference of over 275 end-of-life health professionals, researchers,
policymakers, and community activists, he described the “levers” that could be
used to change the
US
death-denying culture. Bureaucracy would be their ally. Byock noted that “German sociologist Max
Weber said that social movements that become successful become routinized by the
agency of bureaucracy. Therefore,
ironically, bureaucracy is the means and the mark of our success to this
point.” that could be
used to change the
US
death-denying culture. Bureaucracy would be their ally. Byock noted that “German sociologist Max
Weber said that social movements that become successful become routinized by the
agency of bureaucracy. Therefore,
ironically, bureaucracy is the means and the mark of our success to this
point.”
While Byock rallied the ”levers” and “agents
of change,” he also quietly created
a new right-to-die consumer’s group that would organize caregiver and hospice
groups, and pressure legislators to pass living will legislation. Byock brought AAHPM together with Choice
in Dying (aka Euthanasia Society of America and Society for the Right to Die) to
form “Partnership for Caring” (PfC) in 1999. PfC’s mission was to articulate “a
national policy agenda”, and their first priority was “mandated universal access
to high-quality care.”
Just when we think we are supporting a partnership for
caring, we end up with the choice to die.
Now, twelve years later, the Senate is poised to firmly
establish Big Death’s “agency of bureaucracy” by implementing the
Obama/Pelosi/Reid plan.
According to the principle of subsidiarity, medical
decisions should be made at the lowest level – closest to the patient, with the
least bureaucracy. That is the
first step in protecting American health care. All current health “reform”
legislation is the polar opposite.
[i] A core
group from Big Death showed up to support Rep. Blumenauer’s death counseling
bill: AARP,
American Academy of Hospice and Palliative Medicine (AAHPM), American College of
Physicians (ACP), American Hospice Foundation, Center to Advance Palliative Care
(CAPC), Consumers Union, Gundersen Lutheran Health System, Hospice and
Palliative Nursing Association (HPNA), Medicare Rights Center, National Hospice
and Palliative Care Organization (NHPCO), National Palliative Care Research
Center (NPCRC), Providence Health and Services, and Supportive Care
Coalition.
[ii] “HEALTH
REFORM: We Can’t Fix Health Care By (Merely) Fixing Health Care”, August 7,
2009.
|